Classification of ME/CFS patients based on common symptoms
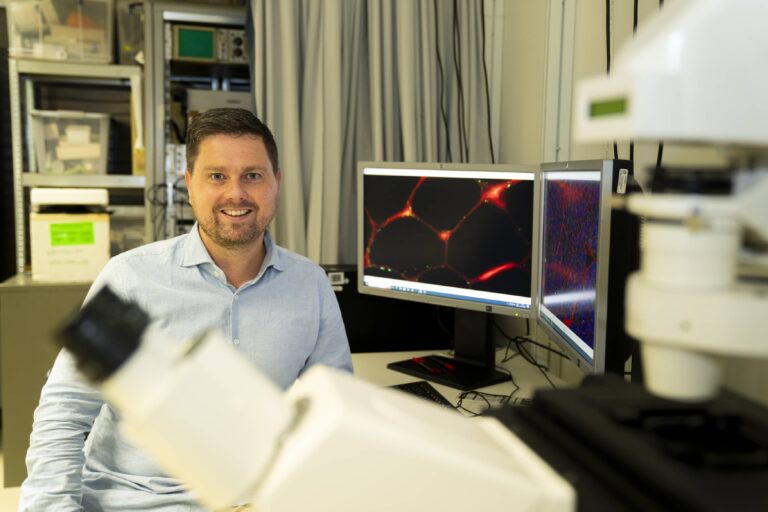
Scientific research among the members of MECVS Nederland, the Dutch national organization for everyone with ME/CFS.
This is an adaptation by MECVS Nederland of the article by Anouk Vaesi and Theo Kuiphof that previously appeared in our magazine.
In addition to profound fatigue, people with ME/CFS experience a wide variety of symptoms, including post-exertional malaise (PEM), sleep problems, pain, and cognitive issues such as concentration and memory problems. These symptoms significantly limit normal daily routines, social life, work, and/or leisure time. As a result, patients experience a reduced quality of life.
Historically, there are over twenty definitions of ME/CFS, each of which includes a distinct set of symptoms. Just four of these definitions are still commonly used. The absence of agreement on a single definition is illustrative for the diversity of the condition. For scientists and doctors, the variation in occurrence and severity of symptoms can be challenging to their research and to support their patients.
Subgroups in the ME/CFS population
There are indications that subgroups of ME/CFS patients exist with similar patterns of severity and frequency of complaints. To gain more insight into these subgroups, ME/CVS Stichting Nederland contributed to a study in collaboration with research clinic Ciro and Maastricht University. The members of ME/CVS Stichting Nederland were invited to complete an online symptom questionnaire. The answers to the questionnaire were also used to determine whether individuals met the criteria of the four most commonly used ME/CFS case definitions:
- Fukuda/CDC criteria (Fukuda);
- Institute of Medicine Criteria (IOM);
- Canadian ME/CFS criteria (CCC);
- ME International Consensus Criteria (ICC).
A thorough approach
Scientists have attempted to classify ME/CFS patients into clusters before. These studies focussed on a limited set of symptoms or used questionnaires who were not scientifically validated. This study used the scientifically validated DePaul questionnaire to collect data on severity and frequency of no fewer than 79 symptoms as experienced by each participant during the last six months. This provided a wealth of information. In addition, the results from this study were compared with the dataset of DePaul University in Chicago, where this questionnaire was developed by Leonard Jason. This makes it the most thorough study of symptoms in ME/CFS to date and led to a publication in the leading scientific Journal of Translational Magazine 1.
Participants in the study
In total, 367 ME/CFS patients completed the questionnaire. We disregarded the 30 participants without an official diagnosis. The 337 persons with an official diagnosis were included in the study. The majority of participants were female, with an average age of 55 years. 55% of participants were married or living with a partner. Approximately two-thirds of participants were unable to work or study.
Scores against the four case definitions
Based on the completed questionnaires, almost 90% of participants met the Fukuda criteria, 80% met IOM, 59% met CCC, and 39% met ICC. The image shows how these groups overlap. More than a quarter of participants met the criteria of all case definitions, while 5% of participants did not meet any of these four. We note that the diagnosis often was made years before this research project. The study does not cover whether someone previously had more or different symptoms that have decreased over time in severity or frequency due to lifestyle adjustments or other ways of symptom management.
The scores against the four criteria sets are interesting. Until now, it was often assumed that the ICC patient group is subgroup of the CCC, which in turn is included in IOM, which itself is largely found within the Fukuda patient population2. However, this study showed that more than a quarter of the ICC group did not meet the CCC criteria and nearly 14% did not meet any other case definition at all.
Post-exertional malaise (PEM) is known as the most characteristic symptom of ME/CFS. PEM is a mandatory symptom in IOM, CCC and ICC, and an optional symptom in Fukuda. In our study, 9 of the 302 participants that met the Fukuda criteria did not experience PEM, which is less than 3% of the “Fukuda-group”. This low number may say more about the habits of the doctors who diagnose ME/CFS rather than about the case definition Fukuda itself. Therefore, we can imagine that this percentage may be different in other countries.
There were 16 participants with an ME/CFS diagnosis who did not meet any of the four case definitions. Of these, 15 were experiencing PEM. One should not exclude them lightly as ME/CFS patients. The scientific publication concludes that inclusion based on one specific criteria set has limited usefulness in scientific research.
The four definitions are not distinguishable enough to accurately divide ME/CFS patients into groups. For that we need to look a step deeper, at the symptoms themselves.
Subgroups of ME/CFS patients based on patterns of symptoms
In addition to profound fatigue and PEM, ME/CFS patients reported a variety of symptoms. A total of 45 clusters of symptoms were identified. The 13 largest clusters consisted of 10 or more people. Here are some examples to give an idea on the clusters. One subgroup was mainly characterized by cognitive complaints, while patients in another subgroup reported more temperature-related complaints and pressure pain. A third group had relatively more problems with disruptions in the day-night rhythm, and less problems with muscle weakness and coordination. There was also a group of patients who stood out for high scores on dizziness and stable standing, combined with extra sensitivity to smells and alcohol. All the clusters found are described in detail in the appendices of the scientific article 1.
There appeared to be no hard dividing line between the groups of clusters. Fatigue and PEM were found in all subgroups. Although all clusters were characterized by a specific pattern of severity and frequency of certain symptoms, this does not mean that these symptoms were not present in the other clusters. The differences between the clusters are mainly about more or less severe or frequent, but they are clearly distinguishable from each other on that basis.
Approximately 11% of the participants could not be classified within one of the 13 larger subgroups. This indicates that a significant proportion of people with ME/CFS has unique patterns of symptoms.
Compare the results with DePaul University
We compared the outcomes with data from DePaul University in Chicago, which has been using the questionnaire for years to collect information on the symptoms of ME/CFS patients. There were differences between the two groups as a whole. For example, on average the patients in the American dataset were younger and their disease burden was generally higher. On average the participants in the American dataset met the criteria of more case definitions. The differences between the two groups is not surprising. The countries have a different healthcare and social system, which affects the chance of getting an ME/CFS diagnosis. The way of recruiting patients was different. In this type of scientific research there is always a selection bias. However, it is interesting that despite these differences, the found cluster classification also applied to the American patient group. This makes it plausible that the found clusters are not a result of social and societal differences, but really contributes to the understanding of ME/CFS.
Discussion and conclusion
The study results show the great variety of symptoms experienced by people with ME/CFS. These findings emphasize the difficulty for healthcare providers to properly guide and treat ME/CFS patients. Which symptom should be addressed first? Can different symptoms be addressed simultaneously? Do symptoms decrease with medication and/or paramedical treatment?
Further research is needed. Biomedical research could reveal associations between impaired body functions and subgroups, and provide more insight into the disease as a whole. Follow-up research could explore the applicability of the clustered subgroups as a means to map day-to-day life. The relationship between subgroups and relevant outcomes for people with ME/CFS, such as quality of life and daily functioning, deserves further investigation. The subgroups and their symptom patterns may serve as a starting point for developing more tailored treatments for ME/CFS patients.
There is still a long way to go. But hopefully the results of this study can help science to move forward a bit in unravelling the mystery of ME/CFS.
* Dr. Anouk Vaes is working as a research associate at Ciro.
[1] Vaes, Van Herck, Deng, Delbressine, Jason, Spruit. Symptom based clusters in people with ME/CFS: an illustration of clinical vatiety in a cross-sectional cohort, J of Translational Medicine 2023, https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-023-03946-6
[2] See for instance: Jason, Kot, Vernon ea. Chronic fatigue syndrome and myalgic encephalomyelitis: towards an empirical case definition, Health psych. and behavioral medecine 2015.



Delen via: